Proximal humerus fracture
Proximal humerus fractures are frequent orthopedic trauma cases, occuring after a low-energy falls in elderly population or after a high-energy trauma for young individuals. Patients present Pain, swelling and decreased motion. an extensive ecchymosis is also present.
Xray is mandatory to classify the fracture, and thus treating it. CT scan is indicated in communitive cases, and sometimes in pre-operative planning.
Generally, non displaced fractures are treated nonoperatively ( Sling immobilisation), whereas displaced fractures need reduction and fixation. Several other variables should be also considered in the therapeutic decision : age, bone quality, dominance, geenral medical condition, concurrent injuries.
Several modalities of Osteosynthesis exist : Plate& screws, Nail, and Percutaneous pinning.
For severly communitive fractures, arthroplasty is indicated ( hemiarthroplasty or reverse total shoulder), allowing faster recovery period.

Plate&screw fixation ( AO surgicalreference)

Orthoinfo-AAOS

Intramedullary nailing ( AO surgicalreference)
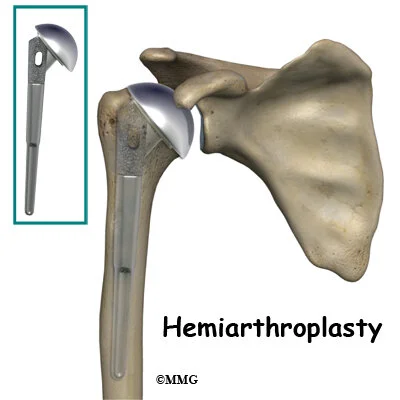
Hemiarthroplasty

Reverse shoulder arthroplasty

4 Fragments in Neer Classification Carofino, B. C., & Leopold, S. S. (2012). Classifications in Brief: The Neer Classification for Proximal Humerus Fractures. Clinical Orthopaedics and Related Research®, 471(1), 39–43. doi:10.1007/s11999-012-2454-9
Some of the risks of surgery of shoulder replacement include infection, wound healing problems, bleeding and injury to nerves and vessels near the fracture. Sometimes the shoulder gets very stiff. Occasionally, the fracture does not heal, and another operation may be recommended.
Clavicle Fracture
Clavicle fractures are frequent and alter the biomechanics of the shoulder
We distinguish 3 zones :
Proximal 1/3 : generally does not need surgery
middle 1/3: surgery is only indicated if
displacement > 100%
neuro vascular complications
cutaneous thread
shortening of at least 2 cm
floating shoulder (clavicle and scapular neck fracture)
Lateral third : surgery is indicated for displaced fracture (relation to ligaments is essential)


Allman classification

How middle 1/3 fractures usually displace
(American family physician website)

Pay attention: Neurovascular …

Lateral Third fracture displacement depends on the integrity of the ligaments

Neer classification for the lateral 1/3 clavicle fractures
Conservative treatment consists of a shoulder immobilizer, with several follow up (skin condition) with Xrays
When surgery is indicated, options are:
plate & screws for middle third or lateral fractures
Arthroscopic repair for lateral third fracture

superior or anterior plate

Hook plate

Arthroscopy for lateral clavicle fracture
Clin Orthop Surg. 2019 Mar;11(1):103-111
Scapula fractures

Generally seen in high energy trauma : search for associated lesions
Many types exists (according to the fractures part)
coracoid fractures
acromial fractures
glenoid fractures
scapular neck fractures
look for associated AC joint separation or clavicle fracture
known as "floating shoulder"
scapular body fractures
described based on anatomic location
scapulothoracic dissociation

Coracoid fracture: type 1 is proximal to coracoclavicular ligaments, type 2 is distal

Acromion fractures:. type1: non or minimally displaced.
type 2: displaced but does not compromise the subacromial space
type3: displaced and comprime the subacromial space

Ideberg classification for scapula fractures
Imaging
Xrays: True AP, scapular Y and axillary lateral view
CT scan usually requested
Treatment
conservative TTT (majority of cases)
surgical treatment
indications
glenohumeral instability
> 25% glenoid involvement with subluxation of humerus
> 5mm of glenoid articular surface step off or major gap
excessive medialization of glenoid
displaced scapula neck fx
with > 40 degrees angulation or 1 cm translation
open fracture
loss of rotator cuff function
coracoid fx with > 1cm of displacement
"double disruption" of the superior shoulder suspensory complex