Elbow Fractures
Distal Humerus Fractures
Distal humerus fractures are traumatic injuries that include
supracondylar fractures
single column (condyle) fractures
bicolumn fractures
coronal shear fractures
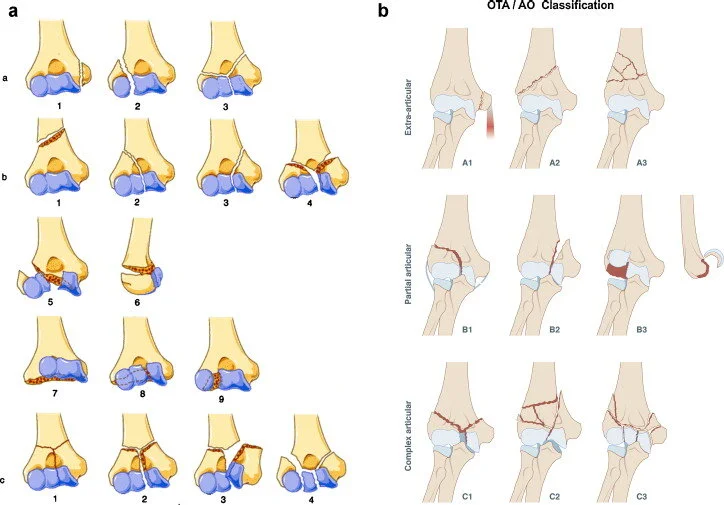
Classification AO/ATO
Type A: Extraarticular (supracondylar fracture),80% are extension type; epicondyle
Type B: Intraarticular-Single column (partial articular-isolated condylar, coronal shear, epicondyle with articular extension)
Type C: Intraarticular-Both columns fractured and no portion of the joint contiguous with the shaft (complete articular)

Distal humerus can be described as 2 columns and a Trochlea
Clinical presentation
Elbow swelling and pain
Gross instability
Always check distal pulse (brachial artery cna be injured) and neurologic exam(radial, ulnar,
and median nerves)
Check for Volkmann syndrome
Imaging
Xrays : AP + Lateral.
FAT PAD sign, if present, shows the presence of infra-radiological fracture
CT scan : for communitive or coronal fracture or articular fracture
MRI : for avulsion fractures in pediatrics ( non ossified)


Xray

Capitellum fracture

CT scan for communitive fracture

MRI for a non ossified avulsion
Treatment
concervative treatment for non displaced fractures with an intact lateral trochlea
Osteosynthesis
Prosthesis ( joint replacement) in communitive fractures in elderly people

Osteosynthesis: perpendicular plating

Osteosynthesis (parallel plating)

Capitellum fracture (coronal fracture)

Prosthesis
Prognosis
Majority of patients regain 75% of elbow motion and strength
Goal is to restore elbow ROM 30-130° of flexion
Unsatisfactory outcomes in up to 25%
treatment of these fractures is complex due to
low fracture line of one or both columns
metaphyseal fragmentation of one or both columns
articular comminution
poor bone quality
Complications may be Elbow stiffness, nonunion, malunion, AIN injury ( with olecranon osteotoomy), Ulnar nerve injury, heterotopic ossification
Radial head fractures
Mechanism of injury: fall on outstretched hand, elbow in extension + forearm in pronation
(most force transmitted from wrist to radial head)
Associated conditions
lateral collateral ligament (LCL) injury (80%)
Medial collateral ligament (MCL) injury
Essex-Lopresti injury
distal radioulnar joint (DRUJ) injury
interosseous membrane disruption
Elbow dislocation
Wrsit / scaphoid fracture

Masson classification : 4 types
Clinical presentation
Pain and stiffness (elbow), especially in prono- suppination
Mechanical blocks
Check forearm and wrist (DRUJ, interosseous membrane)
Check for ligamentous laxity (LCL)
Imaging
Xray AP+ L
CT scan to evaluate communition and displacement
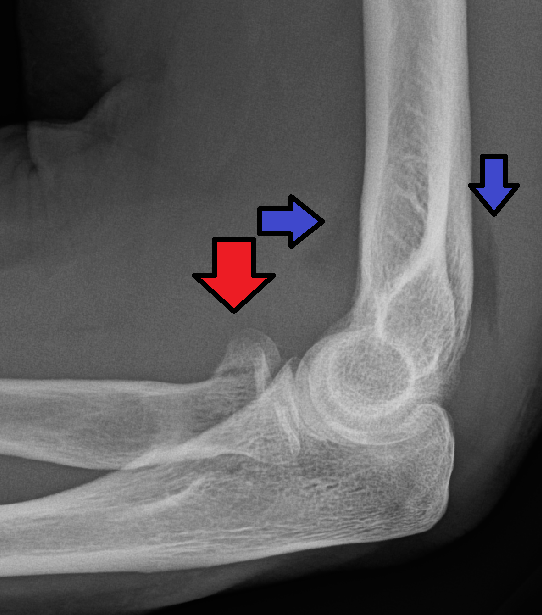
Xray (red arrow)
(blue arrow is for Fat Pad sign)

CT scan
Treatment
Short period of immobilization followed by early ROM ( Mason 1)
Osteosynthesis
Prosthesis for communitive fracture
There is no place in trauma for radial head excision : High rate of instability

Screws

Mini-plate & screws

Prothesis
Potential complications: heterotopic ossifications, stiffness, posterior interosseous nerve damage, infection…..
Olecranon fractures
Olecranon fractures are frequent.
Secondary to a direct blow on the elbow (communitive fractures), or after a fall onto outstretched upper extremity (transverse or oblique)
Treatment
Conservative : immobilisation and begin early mobilisation: in elderly or low demanding patients
Surgical:
Tension band wiring
Intramedullary screw
Plate & screws: communitive fractures
Resection + triceps advancement


Mayo classification

Tension bande wiring

Plate & screws

Intramedullary screw

Resection + triceps advancement
Complications: stiffness, heterotopic ossifications, non union, symptomatic hardware, flessum….