Elbow Dislocation
Posterolateral is the most common type of dislocation (80%)
Usually a combination of
axial loading
supination/external rotation of the forearm
valgus posterolateral force
Pathoanatomic cascade: progression of injury is from lateral to medial
LCL fails first (primary lesion)
by avulsion of the lateral epicondylar origin
midsubstance LCL tears are less common but do occur
MCL fails last depending on degree of energy
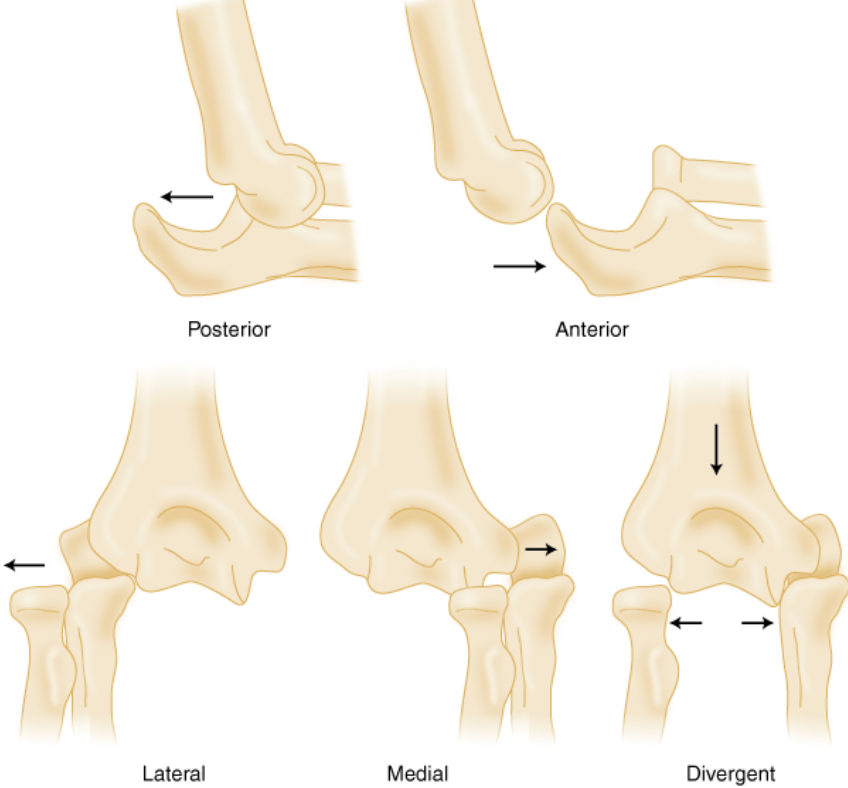
Types of Elbow dislocation
Orthop Clin North Am. 2015 Apr;46(2):271-80
Elbow Stabilizers : Static and dynamic stabilizers confer stability to the elbow
static stabilizers (primary)
ulnohumeral joint
anterior bundle of the MCL
LCL complex (includes the LUCL)
static stabilizers (secondary)
radiocapitellar joint
joint capsule
origins of the common flexor and extensor tendons
dynamic stabilizers
muscles that cross the elbow joint, which apply compressive (stabilizing) force
anconeus
brachialis
triceps


Medial ligament

Lateral ligament
Clinical findings
Pain and swelling
Deformation
Check the status of the skin
Check the presence of compartment syndrome
Check neurovascular status
Check the status of wrist and shoulder
Imaging
Xrays : AP + Lateral
CT Scan: usually after reduction
In front of every elbow dislocation, we must search for Terrible Triade injury which is characterized by:
Elbow dislocation (often associated with posterolateral dislocation or LCL injury )
Radial head or neck fracture
Coronoid fracture
Structures of elbow fail from lateral to medial
LCL disrupted first
anterior capsule injured next
possible MCL disruption

Terrible Triad injury
Treatment : Closed reduction and then assess :
If Stable: splinting at least 90° for 5-10 days, early therapy
If unstable: Operative treatment
If radial head is fractured : Osteosynthesis or prosthesis, but never excision
If elbow remains unstable : repair radial collateral ligament (the most important is the ulnar lateral collateral ligament)
If elbow remains unstable, repair the Coronoid process ( If >10% fractured)
If elbow remains unstable, repair ulnar collateral ligament
If elbow remains unstable, put external fixator (Hinged)
We should alert every patient with an elbow dislocation that it is impossible to regain his full range of motion.