
Thoracolumbar spine
Magerl (AO) classification most used
complete neurologic exam
importance of posterior ligametous complex (PLC)


Type A

Type B

Type C

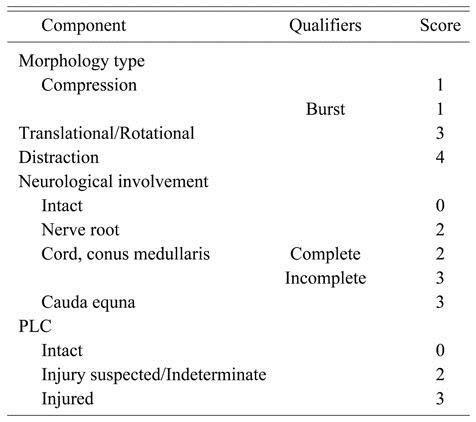
Thoracolumbar Injury Classification and Severity Score (TLICS)
Treatment ( in general)
Type A : kyphoplasty, or posterior instrumentation, or both.
minimally displaced A1 fracture can be treated conservatively (orthosis or functional TTT)
Type B1: posterior instrumentation
Type B2: posterior arthrodesis
type C: arthrodesis
Laminectomy and nerve decompression is only indicated in case of abnormal neurological exam

Hyperextension Brace

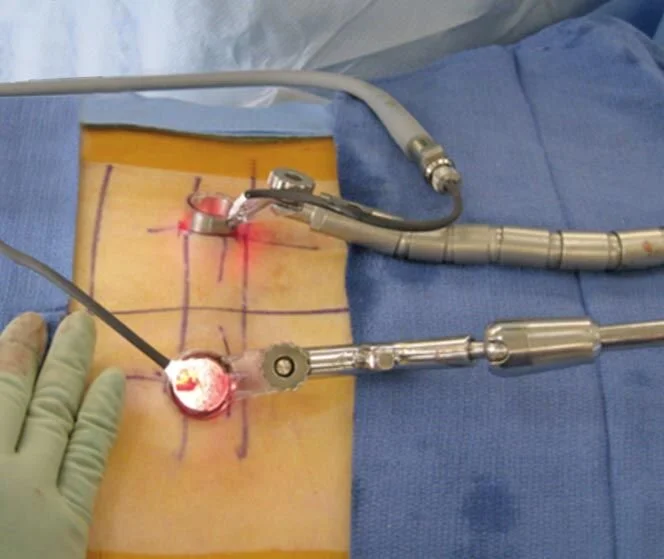
Kyphoplasty

Kyphoplasty

Kyphoplasty + posterior instrumentation
MIS

Advantage of MIS
Cervical Vertebral Fractures
Subaxial
compression fracture ( check posterior ligament complex)
burst fracture (usually neurologic)
Flexion teardrop fracture : TRUE TEAR DROP
characterized by
anterior column failure in flexion/compression
posterior portion of vertebra retropulsed posteriorly
posterior column failure in tension
larger anterior lip fragments may be called 'quadrangular fractures' s
associated with SCI
unstable and usually requires surgery
Extension teardrop avulsion fracture
small fleck of bone is avulsed of anterior endplat (usually C2).
Neurologic exam is normal.
stable “avulsion” : collar

Flexion Tear drop

Tear drop (flexion)

False (extension) tear drop

Facet dislocation ( uni lateral or bilateral)




Locked facet

Atlas Fracture (C1)
risk of neurologic injury is low
commonly missed due to inadequate imaging of occipitocervical junction
Pathophysiology: includes hyperextension, lateral compression, and axial compression
Prognosis : stability dependent on degree of injury and healing potential of transverse ligament
one subtype: Jeffereson’s fracture



Axis Fracture (C2): Hangman’s Fracture
bilateral fracture of pars interarticularis: anterior spondylolithesis.
mechanism: hyperextension
physical exam: Neck pain. Patients are usually neurologically intact



Levine and Edwards Classification
Odontoide Fracture
Odontoid fractures are relatively common fractures of the C2 vertebral body (axis) that can be seen in low energy falls in eldery patients and high energy traumatic injuries in younger patients
Symptoms
neck pain worse with motion
dysphagia may be present when associated with a large retropharyngeal hematoma
Very rare to have myelopathy due to large cross-section area of spinal canal at this level

Anderson and D'Alonzo Classification
