
Avascular necrosis of the lunate leading to abnormal carpal motion
Most common in males between 20-40 years old, with history of trauma
Risk factors
Ulnar negative variance : leads to increased radial-lunate contact stress
Decreased radial inclination
Repetitive trauma
Presentation :
Dorsal wrist pain (Usually activity related, more often in dominant hand)
limited ROM
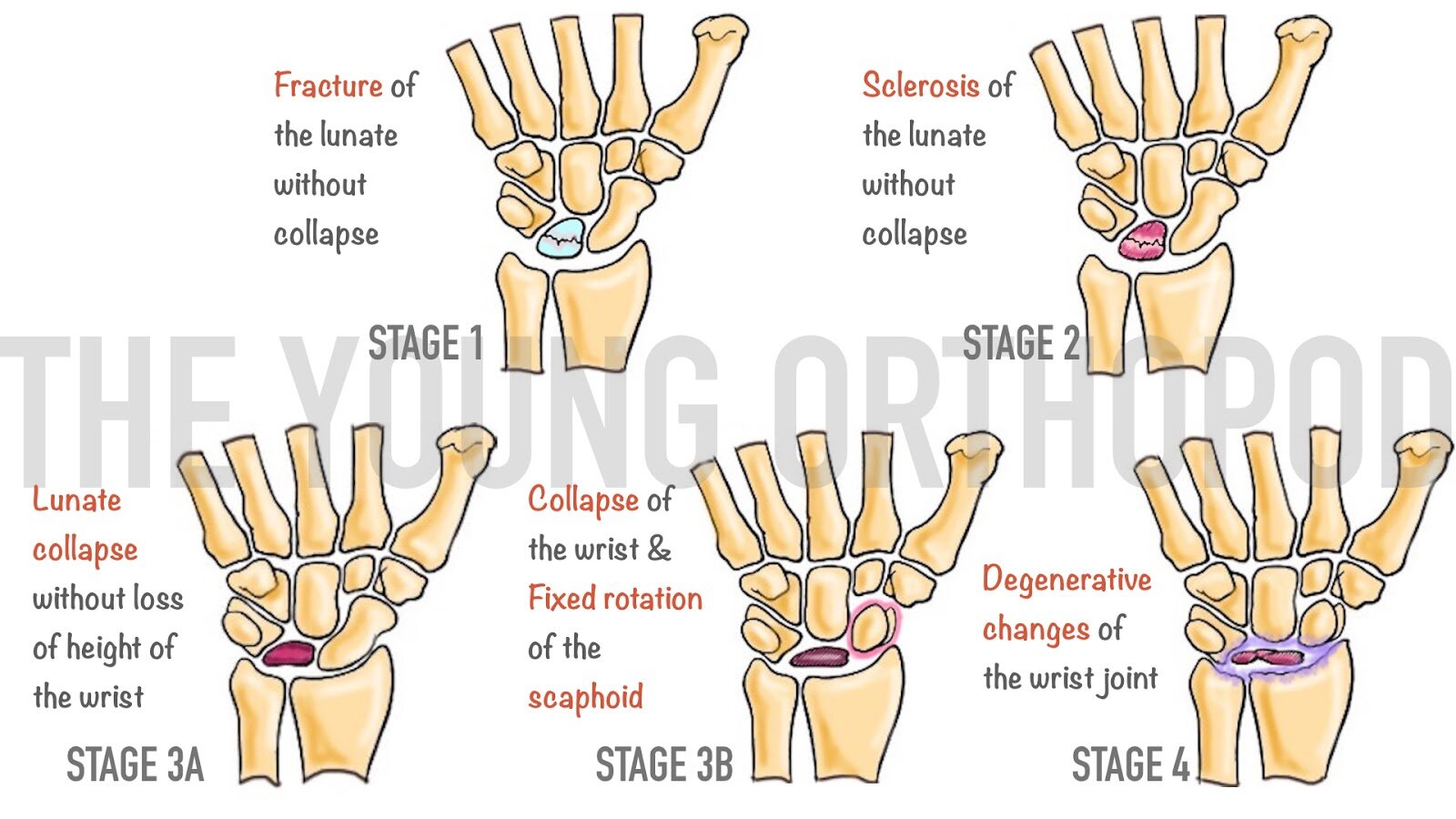

Stage 1

Stage 3A

Stage 2

Stage 3B

Stage 4
Imaging:
Xrays are needed, bilateral
Scan: useful when collapse occurs
MRI: for early detection (Decreased T1 signal)
Treatment:
Conservative
Cast + NSAIDs : onbly for stage 1 patients. BUT later procedures are often needed.
Operative
Temporary scaphotrapeziotrapezoidal pinning : in adolescent with radiographic evidence of Kienbock’s and progressive wrist pain
Joint leveling procedure ( radial shortening)
Stage I, II, IIIA disease with ulnar negative variance
Radial wedge osteotomy
Stage I, II, IIIA disease with ulnar positive or neutral variance
Vascularized bone grafts: stage I to IIIB. Needs long term results
Core decompression: stage I, II ad IIIA
Partial wrist fusions
STT
capitate shortening osteotomy +/- capitohamate fusion
scaphocapitate
indications
Stage II disease with ulnar neutral or positive variance
Stage IIIA or IIIB disease
must address internal collapse pattern (DISI)
Proximal row carpectomy (PRC) : stage IIIB or IV
Wrist fusion : stage IV
Total wrist arthroplasty: stage IV

Radial shortening

Radial Wedge osteotomy

Proximal row carpectomy
