Sports Hernia (Atheletic Pubalgia)
Pubalgia is a fairly uncommon condition seen chiefly in young athletes.
males > females
common in hockey players and soccer players
Also known as athletic pubalgia, sportsman’s hernia, sports hernia, Gilmore’s groin, pubic inguinal pain syndrome-PIPS, sportsmen’s groin, footballer’s groin injury complex, hockey player’s syndrome, athletic hernia…
At least three of the five clinical findings should be present to make a diagnosis of sportsman’s hernia, i.e.:
1) Point sensitivity where the conjoint tendon adheres to the public tubercle
2) Sensitivity to palpation in the deep inguinal ring
3) Pain and/or dilation in the outer inguinal ring without apparent hernia
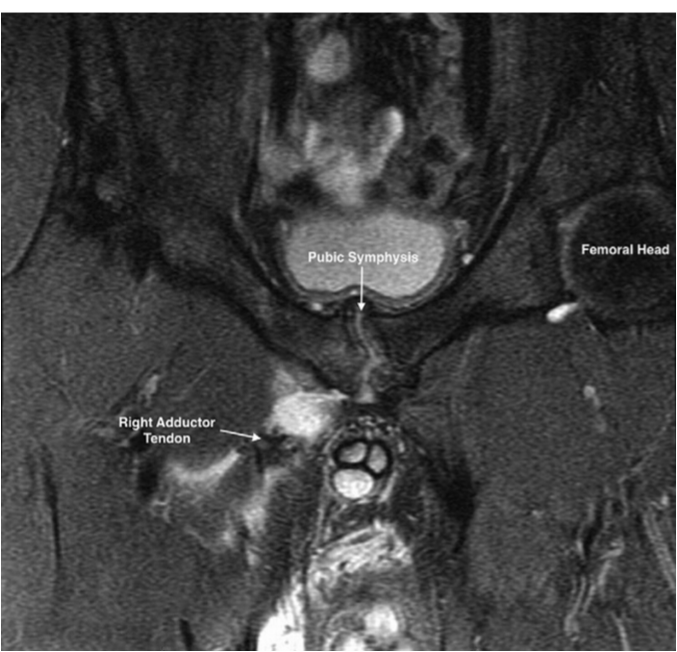
4) Pain at the origin of adductor longus muscle
5) Diffuse inguinal pain extending to the perineum, inner surface of the femur and crossing the midline
French Orthopedics have devided the Atheletic pubalgia into 3 groups
Abdominal level:
Attachement or the rectus abdominalis (abdominal aponeurosis)
A sports hernia does not cause a visible bulge in the groin, like the more common, inguinal hernia does. Over time, a sports hernia may lead to an inguinal hernia. With sportsman’s hernia, the posterior wall of the inguinal canal (transversalis fascia) is weak. Some sportsmen also present with disruption of the aponeurosis of the external oblique muscle.
Inguinal and/or genital neuropathy .
Muschaweck and Berger [21] postulated that pressure on the genital femoral nerve from the bulging posterior inguinal floor can be a source of pain. As a result, selective resection of the genital nerve is performed as a part of their repair
Symphysis level: degenerative changes
Adductor level : tendinopathy or avulsion
Symtoms: The primary symptom is exercise-related inguinal pain. The pain is typically localized on the lower lateral end of the rectus abdominis muscle and it may extend to the testicle, perineum, suprapubic region, origin of adductor longus and inner surface of the femur




The pubic aponeurosis is created by the confluence of the rectus abdominus, the conjoint tendon (a fusion of the internal oblique and transversus abdominus), and the external oblique. This pubic aponeurosis is also confluent with the origin of the adductor and gracilis, the combination of which is termed the rectus abdominus/adductor aponeurosis


Matalon, S. (2017). Don’t Forget the Abdominal Wall: Imaging Spectrum of Abdominal Wall Injuries after Nonpenetrating Trauma. RadioGraphics, 37(4), 1218–1235.

Matalon, S. (2017). Don’t Forget the Abdominal Wall: Imaging Spectrum of Abdominal Wall Injuries after Nonpenetrating Trauma. RadioGraphics, 37(4), 1218–1235.

Matalon, S. (2017). Don’t Forget the Abdominal Wall: Imaging Spectrum of Abdominal Wall Injuries after Nonpenetrating Trauma. RadioGraphics, 37(4), 1218–1235.
Differential diagnosis

Imaging

Osteolysis

Ossification of the adductor tendon

Adductor tendon avuslion
Brennan 2005. Secondary Cleft Sign as a Marker of Injury in Athletes with Groin Pain: MR Image Appearance and Interpretation. Radiology, 235(1), 162–167.

Cleft sign
Brennan 2005. Secondary Cleft Sign as a Marker of Injury in Athletes with Groin Pain: MR Image Appearance and Interpretation. Radiology, 235(1), 162–167.

Cleft sign + avulsion of gracilis
Brennan 2005. Secondary Cleft Sign as a Marker of Injury in Athletes with Groin Pain: MR Image Appearance and Interpretation. Radiology, 235(1), 162–167.
Brennan 2005. Secondary Cleft Sign as a Marker of Injury in Athletes with Groin Pain: MR Image Appearance and Interpretation. Radiology, 235(1), 162–167.

Arthro- MRI showing the secondary cleft sign
Dynamic ultrasonography is a promising method for the diagnosis of sportsman’s hernia. A radiologist with plenty of experience in ultrasonography may identify the significant protrusion of transverse fascia during Valsalva maneuver using a high-frequency probe (Figure 3) (30). Slight bulge in the posterior inguinal wall may often be asymptomatic

Treatment
First line Treatment : NSAIDs, Rest, Physical therapy, injection if enthesopathy (steroids vs steroids)
Surgery is indicated if conservative treatment fails

Hopkins, J. N., Brown, W., & Lee, C. A. (2017). Sports Hernia. JBJS Reviews, 5(9), e6. doi:10.2106/jbjs.rvw.17.00022

External oblique aponeurosis weakness and thinning in an athlete undergoing athletic pubalgia surgery


Physiotherapy
British Hernia Society’s 2014 position statement based on the Manchester Consensus Conference
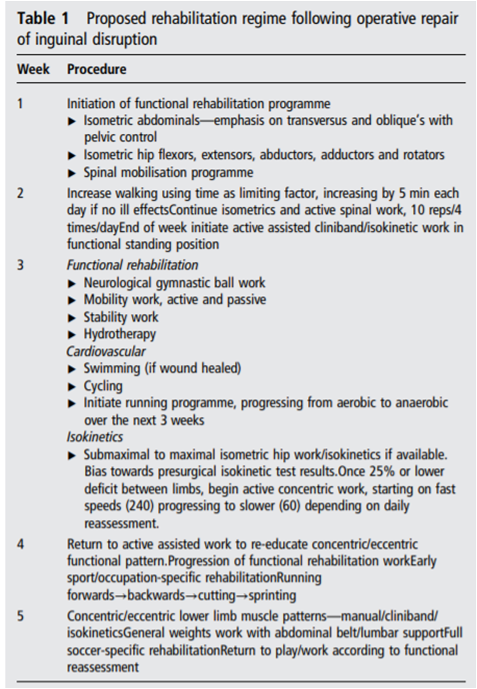
Physiotherapy
British Hernia Society’s 2014 position statement based on the Manchester Consensus Conference